
As for a lot (or most) conditions we treat with antimicrobials in dogs and cats, data on how best to use antimicrobials before, during and after dental procedures are sparse. We know that antimicrobials are used a lot for canine and feline dental procedures (Weese et al. 2023), and that a large percentage of said use is probably unnecessary. The same is true in human dentistry; even though they have more data and more guidelines, they still struggle with overuse and poor compliance with best practices.
Part of guideline development is assessing the available evidence. Even when we know evidence is lacking, we still want to assess the issue carefully to makes sure there isn’t more evidence than we thought, and to critically assess what little data may be present to help highlight knowledge gaps.
We recently completed a systematic review of infectious complications of dental procedures in dogs and cats, and the impact of antimicrobial prophylaxis (Weese et al. 2026). Specifically, we addressed a series of questions about use of antimicrobials for routine dental procedures, looking at both peri-procedural (i.e. shortly before and up to 24 hours after the procedure) and post-procedural (i.e. more than 24h after the procedure) antimicrobial administration.
- Unsurprisingly, we found that data were really limited. That’s important itself. It’s a gap that needs to be filled.
- We also found that studies rarely looked at (and were rarely well designed to look at) the key outcomes we care about, i.e. clinical disease. We settled on looking at sepsis, infective endocarditis, local tissue infection and adverse events as the critical outcomes.
- After some debate, we also included bacteremia (bacteria in the bloodstream) as an outcome of interest, even though it’s not a clinical outcome. Bacteremia is a state that may or may not be associated with disease. People and animals are regularly bacteremic and typically have no consequences from it at all. However, bacteremia can progress to infection in rare circumstances. We wouldn’t normally use a non-clinical outcome like that (especially one that is as common as bacteremia), but most of the comparative studies in dogs and cats focused on bacteremia. So we included it, recognizing the limitations.
The systematic review highlighted the commonness of bacteremia associated with dental procedures, as shown in the figure below of the meta-analysis. The proportion column is the prevalence of bacteremia associated with dental procedures in each study, and the pooled prevalence across studies was 47%.
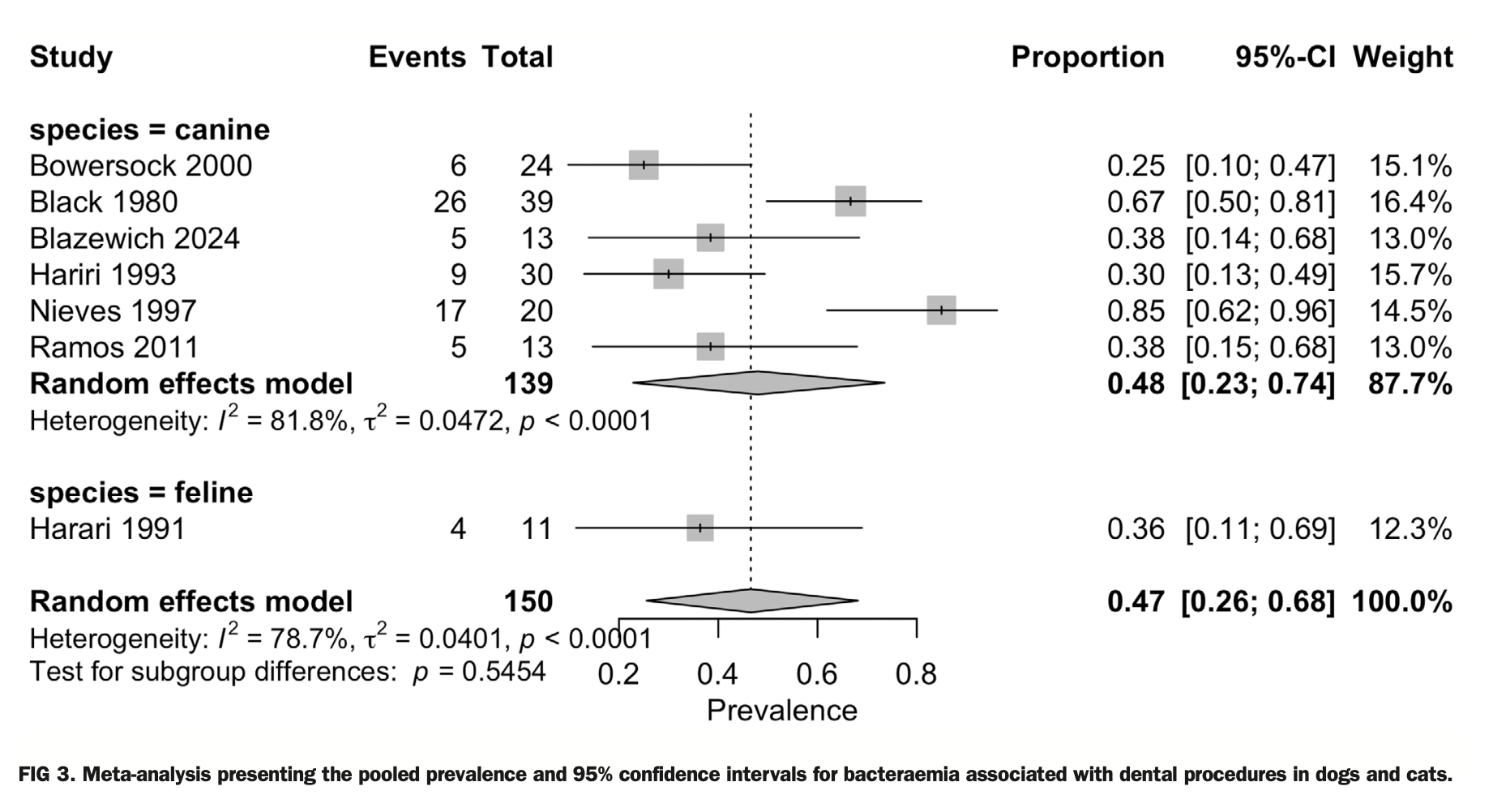
These studies didn’t report clinical consequences of bacteremia, but when you consider how many dogs and cats undergo dental procedures, the really high bacteremia rates and the really low apparent incidence of dogs and cats getting sick after their procedures, you can understand how bacteremia (seemingly not a big deal) is not a good proxy for clinical disease (which is a big deal).
To investigate this further, we asked whether dental-associated bacteremia is associated with sepsis, endocarditis or other infectious consequences. Only two studies looked at this. Both were small (total of 22 dogs with bacteremia and 11 without) and no infectious consequences or disease were noted in these animals. The data were so limited we couldn’t evaluate them further or draw any conclusions.
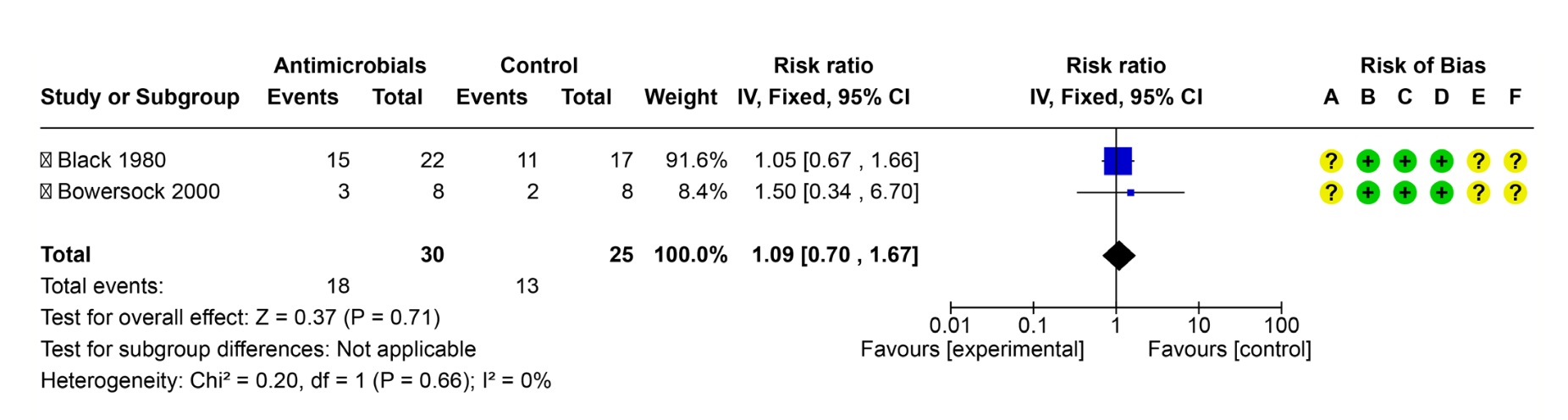
We then asked “In dogs and cats undergoing dental procedures, does peri-procedural administration of antimicrobials reduce the incidence of endocarditis, sepsis, bacteremia or other infectious complications?” But no studies looked at these clinical outcomes. Only two small studies looked at the effects on the incidence of bacteremia, and the meta-analysis (see below) didn’t suggest there was any beneficial effect. The certainty of evidence was really low of course, based on a variety of factors.
That doesn’t mean we can say antimicrobials for dental procedures don’t have any effect, it just means we have nothing suggesting they do. If we look at human dentistry where there are stronger data, antimicrobials are not indicated for these procedures, apart from in certain high risk patients. Our lack of identified effect has to be tempered because the data are weak, but there’s also nothing suggesting antimicrobials are needed (or useful) for routine veterinary dental procedures in most patients.
If there’s no evidence that peri-procedural antimicrobials are useful, there’s even less reason to think that post-procedural antimicrobials are useful, yet this is commonly done in veterinary and human dentistry. We aimed to address the question “In dogs and cats undergoing dental procedures, does post-procedural administration of antimicrobials reduce the incidence of endocarditis, sepsis, bacteraemia or other infectious complications?” There were no data for this at all. If we look at data and guidelines from human dentistry, routine post-procedural antimicrobials are not typically recommended, or useful.
Did this review actually tell us anything? Yes and no. I think we ended up with the conclusions we were expecting, i.e. bacteremia is commonly associated with dental procedures, there’s no evidence that antimicrobials are useful for routine dental procedures, and the data are really limited.
The fact that we have no supporting evidence for routine use of antimicorbials for dental procedures was an important finding in this case. When we have an intervention (i.e. antimicrobial use) that has potential harms (e.g. cost, adverse events like diarrhea, selection for antimicrobial resistance, administration challenges, pain from administering a pill to an animal with a sore mouth), the default ought to be not to use it unless we have compelling data or a plausible reason to think that the benefits outweigh the harms. For the routine veterinary dental procedures, we have no such data or reason to justify routine antimicrobial use.